Abstract
Background: Malnutrition is an important clinical problem associated with increased morbidity, mortality, and prolonged hospital stay. However, nursing students’ knowledge and preparedness regarding clinical nutrition are often reported to be insufficient. This study aimed to evaluate the effect of a Nutrition Nursing course, delivered under the leadership of a nutrition nurse and based on the Practice-to-Academia educational model, which aims to transfer clinical experience into academic education, on nursing students’ clinical nutrition knowledge.
Methods: This quasi-experimental study was conducted with third-year nursing students enrolled in the Nutrition Nursing course in the nursing department of a university during the 2023–2024 academic year. Data were collected using a Descriptive Information Form and a 25-item Nutrition Knowledge Test. A pre-test was administered at the beginning of the course and a post-test after the 15-week training period. Data were analyzed using SPSS 27.0, and pre-test–post-test comparisons were performed using the Wilcoxon Signed-Rank Test.
Results: Following the educational program, a significant increase was observed in students’ nutrition knowledge across all major domains (p < 0.001). The greatest improvement was identified in the domain of basic concepts of clinical nutrition therapy. Significant increases were also observed in knowledge related to malnutrition screening, clinical nutrition therapy practices, and nursing responsibilities.
Conclusion: A clinically oriented educational program led by a nutrition nurse and based on the Practice-to-Academia model significantly improves nursing students’ knowledge of clinical nutrition therapy.
Keywords: clinical nutrition education, nutrition nursing, malnutrition screening, nursing students, Practice-to-Academia model
Main Points
- Education led by a nutrition nurse improved nursing students’ clinical nutrition knowledge.
- The Practice-to-Academia model integrated clinical experience into nursing education.
- Knowledge levels improved in malnutrition screening and clinical nutrition therapy.
Introduction
Malnutrition is a prevalent and significant clinical problem associated with increased morbidity, mortality, and prolonged hospital stays.1,2 European Society for Clinical Nutrition and Metabolism (ESPEN) provides guidance on clinical nutrition therapy, nutritional care processes, enteral feeding practices, and the identification and management of nutrition-related problems, thereby supporting healthcare professionals in delivering evidence-based nutritional care.1
Therefore, adequate preparedness in clinical nutrition should be considered one of the core professional competencies in nursing education.3-5 However, existing studies indicate that nursing students’ knowledge and preparedness regarding clinical nutrition practices need further development.5-7 Furthermore, review and scoping studies emphasize that nutrition education at the undergraduate level is often limited in scope and predominantly theoretical, which may create a persistent gap between knowledge acquisition and clinical practice.8,9
Competence in clinical nutrition cannot be achieved through theoretical instruction alone; it requires contextual learning integrated with real clinical decision-making processes. Patricia Benner’s Novice to Expert model10 emphasizes that clinical competence develops through experiential learning, progressing from rule-based knowledge to contextual and intuitive clinical reasoning. This theoretical framework suggests that the active involvement of experienced clinicians in the educational process may facilitate students’ deeper and more practice-oriented understanding of clinical knowledge.6,11,12
Within this context, a model led by nurses and integrating clinical experience into undergraduate education may provide an important approach to bridging the gap between theory and practice.5 Experiential learning is particularly critical in areas such as malnutrition assessment and the appropriate management of clinical nutrition therapy, which directly influence patient outcomes.13Therefore, the present study aimed to evaluate the effects of a nutrition nurse–led educational model on undergraduate nursing students’ readiness for clinical nutrition and their knowledge gain.
Methods
Study participants
The study population consisted of all third-year nursing students (n = 48) enrolled in the Nutrition Nursing course at Nuh Naci Yazgan University during the 2023–2024 academic year. Since all eligible and volunteer students were included in the study, a census sampling method was used. The Nutrition Nursing course is offered as an elective course within the undergraduate nursing curriculum. Students who did not participate in either the pre-test or post-test, withdrew from the study at any stage, or submitted questionnaires containing incomplete or invalid data were excluded from the analysis. Sample size was calculated using G*Power 3.1.9.7 based on the difference between two dependent means. Assuming a two-tailed test, an effect size of
dz = 0.50, α = 0.05, and a statistical power of 0.80, the minimum required sample size was determined to be 34. The study was completed with 48 participants, indicating that the sample size was adequate.
Data collection
The data collection tool was developed by two nurses with over 10 years of experience in the field of nutrition nursing and three faculty members holding PhD in nursing. During the development of the data collection tools (pre-test and post-test), expert opinions were obtained from two nutrition nurses certified by the Republic of Türkiye Ministry of Health (RTMH), each with more than 10 years of professional experience in nutrition nursing. One of these nutrition nurses also served as the course instructor and was responsible for designing the Practice-to-Academia model. The instructor holds a PhD in Internal Medicine Nursing, a Nutrition Nurse certification from the RTMH, and an ESPEN Lifelong Learning (LLL) teaching certificate. This nurse is an educator who applies the applied academy model.
Of the three faculty members involved in the development of the data collection tool, two are Associate Professors and one is an Assistant Professor; all are affiliated with the Faculty of Nursing and have over 20 years of academic experience in nursing.
The data collection tool consisted of two sections. The first section, the Descriptive Information Form, included 10 sociodemographic questions covering variables such as age, gender, grade point average (GPA) and whether the student had previously received nutrition education.
The second section included the Nutrition Knowledge Test (Appendix 1) which consisted of 25 multiple-choice questions, each with five options and one correct answer. The test content covered topics such as basic principles of nutrition and functions of nutrients, energy balance and food groups, nutrition in special populations (e.g., infants, older adults, pregnant women), clinical nutrition (e.g., diabetes, coronary heart disease, obesity), as well as nutrition assessment and patient education. Each correct answer was scored as 1 point, and the total score ranged from 0 to 25.
The data collection process was conducted face-to-face in the classroom under the supervision of the researchers. The procedure was carried out in two stages. The pre-test was administered in the first week of the semester following the course introduction, during which both the Descriptive Information Form and the Nutrition Knowledge Test were completed. The post-test was administered after the completion of the 15-week course period, during which only the Nutrition Knowledge Test was re-administered.
Educational process
Within the undergraduate nursing curriculum, students are generally provided with nutrition education covering fundamental concepts such as nutrients, nutritional requirements, and nutrition across different life stages. However, this education is predominantly theoretical, and limited emphasis is placed on clinical nutrition practices. Prior to this study, although students had been exposed to basic nutrition content, structured and nurse-led training specifically focused on clinical nutrition therapy had not been provided.
It is stated that the instructor responsible for delivering the course actively serves as a nutrition nurse and holds a PhD in Nursing. The instructor is certified in nutrition nursing RTMH and possesses an ESPEN LLL teaching certification. Furthermore, it is emphasized that the instructor developed the Practice-to-Academia model based on academic and clinical experience in the field of nutrition nursing and made significant contributions to both its theoretical framework and practical implementation.
The educational intervention consisted of a Nutrition Nursing course conducted over a period of 15 weeks, with two hours of instruction per week, as part of the undergraduate nursing curriculum. The course content was developed in accordance with the curriculum framework of the Council of Higher Education14 and international standards such as those proposed by the American Association of Colleges of Nursing.15 The educational program was designed based on the Practice-to-Academia approach, aiming to integrate clinical experience into the academic learning process.
Teaching methods included lectures, clinical case analyses, case discussions, question–answer sessions, interactive discussions, and examples based on real clinical experiences. Students were encouraged to reflect on cases related to clinical nutrition management and to develop evidence-based nursing practices.
Statistical analyses
Data were analyzed using IBM SPSS Statistics version 27.0. Prior to analysis, data were checked for completeness and consistency. Categorical variables were presented as number (percentage), and continuous variables were presented as mean ± standard deviation (SD). Normality was assessed using the Shapiro–Wilk test. Since the distribution of nutrition knowledge scores did not meet normality assumptions (p < 0.001), non-parametric tests were applied. Pre-test and post-test scores were compared using the Wilcoxon Signed-Rank Test. Comparisons of knowledge scores across descriptive characteristics were performed using the Mann–Whitney U test (for two groups) or the Kruskal–Wallis test (for three or more groups). A p-value of < 0.001 was considered statistically significant.
Results
The descriptive characteristics of the students are presented in Table 1. The majority of participants were female 83.3%, and 66.7% were between 20 and 22 years of age. Approximately two-thirds 68.8% had no prior formal education related to nutrition, and 62.5% of the students expressed interest in receiving additional clinical nutrition training.
| Values are presented as number (percentage). | ||
| Table 1. Descriptive characteristics of the students (n = 48) | ||
| Variable |
|
|
| Age (years) | ||
| 18–19 (n=16) |
|
|
| 20–22 (n=32) |
|
|
| Gender | ||
| Female |
|
|
| Male |
|
|
| Previous Education on Nutrition | ||
| No |
|
|
| Yes |
|
|
| Willingness to Receive Clinical Nutrition Training | ||
| Yes |
|
|
| No |
|
|
The comparison of Nutrition Knowledge Test scores by descriptive characteristics is presented in Table 2. A statistically significant increase was observed in overall nutrition knowledge scores following the course (p < 0.001). A significant difference was found across age groups (p = 0.041), with greater score increases in students aged 20–22 years (+26.57) compared to those aged 18–19 years (+23.62). No significant differences were found according to gender (p = 0.612) or prior nutrition education (p = 0.303). Although not statistically significant, higher score increases were observed in students willing to receive additional training (+28.40 vs. +21.30; p = 0.090).
| *Comparisons between two groups were performed using the Mann–Whitney U test, and comparisons among three or more groups were performed using the Kruskal–Wallis test. | ||||
| Table 2. Comparison of nutrition knowledge test scores by descriptive characteristics (n = 48) | ||||
| Variable |
Mean ± SD |
Mean ± SD |
|
|
| Age (years) | ||||
| 18–19 |
|
|
|
|
| 20–22 |
|
|
|
|
| Gender | ||||
| Female (n=40) |
|
|
|
|
| Male (n=8) |
|
|
|
|
| Previous Nutrition Education | ||||
| Yes (n=15) |
|
|
|
|
| No (n=33) |
|
|
|
|
| Willingness to Receive Clinical Nutrition Training | ||||
| Yes (n=30) |
|
|
|
|
| No (n=18) |
|
|
|
|
The pre-test and post-test comparisons of the Nutrition Knowledge Test domains are presented in Table 3. Across all five knowledge domains, statistically significant differences were observed between pre-test and post-test mean scores (p < 0.001). The largest improvement was observed in the basic concepts of clinical nutrition therapy domain (Δ = −0.37), followed by clinical nutrition therapy applications (Δ = −0.27) and malnutrition risk screening (Δ = −0.26). The smallest improvement was observed in the complications domain (Δ = −0.15)
| * Comparisons were analyzed using the Wilcoxon Signed-Rank Test. Negative values indicate improvement in knowledge scores. | ||||
| Table 3. Nutrition knowledge test domains pre-test and post-test comparisons | ||||
| Category |
|
|
|
|
| Basic concepts in clinical nutrition therapy |
|
|
|
|
| Malnutrition risk screening |
|
|
|
|
| Clinical nutrition therapy applications |
|
|
|
|
| Nursing care in clinical nutrition therapy |
|
|
|
|
| Complications in clinical nutrition therapy |
|
|
|
|
Table 4 includes the pre-test and post-test statistics for the analysis of the Nutrition Knowledge Test subdomains. At the subdomain level, the largest changes were observed in nutrition indications (Δ = −0.48), enteral nutrition products (Δ = −0.44), and indicators of malnutrition (Δ = −0.46) (p < 0.001). No statistically significant differences were found in evaluation of treatment efficacy (Δ = −0.04, p = 0.157) or gastrointestinal complications (p = 1.000). Detailed results are presented in Table 4.
| * Comparisons were analyzed using the Wilcoxon Signed-Rank Test. Negative values indicate improvement in knowledge scores. | ||||
| Table 4. Pre-test and post-test statistics for nutrition knowledge test subdomains analysis. (n = 48) | ||||
| Questions |
Mean ± SD |
Mean ± SD |
|
|
| Basic Concepts in clinical nutrition therapy | ||||
| Nutrition organizations |
|
|
|
|
| Nutrition indications |
|
|
|
|
| Enteral nutrition products |
|
|
|
|
| Use of parenteral nutrition products |
|
|
|
|
| Principles of parenteral nutrition |
|
|
|
|
| Malnutrition risk screening | ||||
| Definition of malnutrition |
|
|
|
|
| Purpose of screening |
|
|
|
|
| Nutritional screening tools |
|
|
|
|
| Indicators of malnutrition |
|
|
|
|
| Timing of screening |
|
|
|
|
| Clinical nutrition therapy applications | ||||
| Nutritional requirements and calculations |
|
|
|
|
| Preparation and administration of nutrition solutions |
|
|
|
|
| Evaluation of treatment efficacy |
|
|
|
|
| Indications for enteral/parenteral nutrition |
|
|
|
|
| Routes of clinical nutrition therapy |
|
|
|
|
| Nursing care in clinical nutrition therapy | ||||
| Basic nursing responsibilities in clinical nutrition therapy |
|
|
|
|
| Communication and collaboration in nutrition care |
|
|
|
|
| Monitoring and documentation of clinical nutrition therapy |
|
|
|
|
| Maintaining sterility and line care |
|
|
|
|
| Assessment of patient tolerance to clinical nutrition therapy |
|
|
|
|
| Complications in clinical nutrition therapy | ||||
| Prevention of complications |
|
|
|
|
| Early detection of complications |
|
|
|
|
| Gastrointestinal complications |
|
|
|
|
| Metabolic and mechanical complications |
|
|
|
|
| Nursing responsibilities in complication management |
|
|
|
|
Discussion
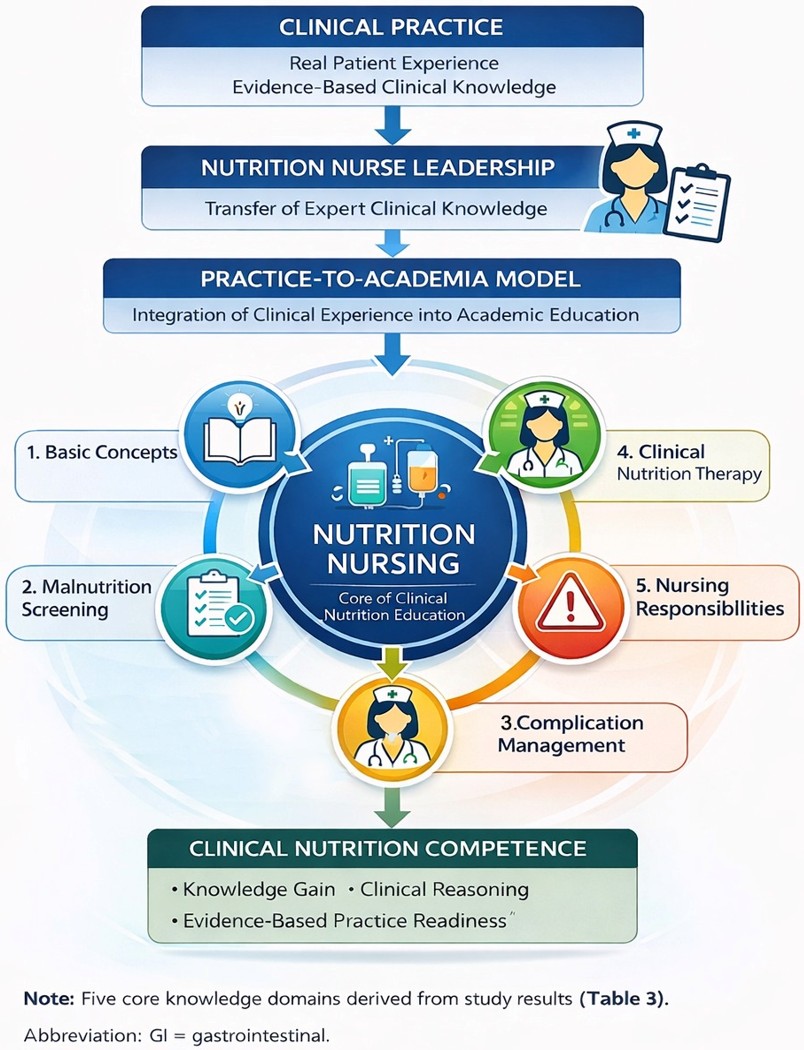
This study demonstrated that a nutrition nursing program conducted under the leadership of a nutrition nurse significantly improved nursing students’ nutrition knowledge across all major domains, including basic concepts of clinical nutrition therapy, malnutrition risk screening, clinical nutrition therapy practices, nursing responsibilities, and complication management. The magnitude and consistency of the pre-test–post-test gains observed across nearly all subcategories indicate that targeted nutrition education can effectively address the well-documented knowledge gaps among nursing students. These findings are also consistent with the Practice-to-Academia Clinical Education Model developed in this study (Figure 1). Within this model, experience and evidence-based knowledge derived from clinical practice are transferred into the academic environment through a structured educational program led by a nutrition nurse.
Previous studies have shown that blended learning approaches supported by real-life clinical scenarios significantly improve students’ knowledge and nutrition counseling skills.16 These findings are consistent with the results of the present study and support the effectiveness of structured educational programs. Moreover, integrating academic knowledge with clinical practice through academia–clinical collaboration has been reported to enhance clinical competencies and professional development.17 In this context, the structured, case-based educational approach implemented in this study is considered to have contributed to both knowledge acquisition and the transfer of knowledge into clinical practice, in line with the Practice-to-Academia model.
Consistent with previous studies, these findings confirm that nursing students often begin undergraduate programs with limited knowledge of nutrition and benefit substantially from structured educational interventions. Systematic and scoping reviews have shown that nursing students generally have insufficient baseline knowledge in both basic nutrition and clinical nutrition.5,8 Similarly, the substantial knowledge gains observed after the course in this study support the view that nutrition education should be considered a core professional competency rather than a supplementary topic within nursing curricula.6,14,15
Significant improvements were also observed in knowledge related to malnutrition screening.16 In particular, notable gains were found in students’ understanding of indicators of malnutrition, screening tools, and the purposes of screening.17 These findings are highly consistent with Bauer et al.18, who reported that malnutrition knowledge among nursing students is generally at a moderate level and emphasized the importance of active teaching methods. Early identification of malnutrition is one of the fundamental responsibilities of nurses within the clinical care process. Therefore, adequate knowledge of screening tools is critical for the implementation of evidence-based nutritional care. Similarly, Ibrahim and Aldawsari19 emphasized that strong nutrition knowledge forms the foundation for nurses’ ability to apply evidence-based screening practices. The findings of the present study suggest that focused educational interventions can significantly strengthen students’ ability to recognize nutritional risk.20
Significant improvements were also observed in knowledge related to nursing responsibilities in clinical nutrition therapy. Increases in students’ knowledge regarding patient monitoring, documentation, sterility, assessment of patient tolerance, and interdisciplinary communication indicate that the educational program enhanced awareness of clinical responsibilities. These findings are consistent with studies showing that structured nutrition education improves both knowledge and practice-related behaviors.21 In addition, Dogan et al.8 emphasized that addressing nutrition within both academic and clinical learning environments is essential to prepare nursing students for real-world clinical care settings.
One of the key strengths of this study is that the educational program was conducted by a nutrition nurse with clinical experience. Nutrition nurses play an active role in the assessment of malnutrition risk, planning of clinical nutrition therapy and patient monitoring. Therefore, transferring clinically grounded knowledge into the educational process may significantly contribute to the development of students’ professional competencies in nutrition care. In this context, education programs led by nutrition nurses may represent an effective approach to improving nursing students’ knowledge and clinical readiness in clinical nutrition.
Furthermore, this study is important as it represents the first empirical evaluation in Türkiye of an undergraduate nutrition nursing course led by a nutrition nurse. Considering that nutrition topics are often addressed only to a limited extent within nursing education in Türkiye, evaluating structured educational models of this kind may contribute significantly to both the development of educational programs and the strengthening of clinical nutrition care.
This study has several limitations. The fact that the research was conducted at a single center limits its generalizability. Furthermore, evaluating only short-term effects restricts the ability to draw conclusions about long-term outcomes. A limitation of these services is the exclusion of questions related to clinical treatment and drug administration, which are frequently encountered in the clinical settings of the researchers.
Conclusion
This study demonstrated that an educational program led by a nutrition nurse and integrating clinical experience into academic education significantly improves nursing students’ knowledge of clinical nutrition therapy. The findings indicate that educational approaches focused on key areas of clinical care, particularly malnutrition screening and clinical nutrition therapy, can effectively enhance nursing students’ competencies in clinical nutrition therapy.
Ethical statement
The study was approved by the Scientific Research and Publication Ethics Committee of Nuh Naci Yazgan University (Approval No: 2024/002-05, Approval date: 12.02.2024). All participants were informed about the study and provided voluntary consent prior to participation.
Acknowledgements
The authors would like to express their sincere gratitude to all participants and clinical staff who supported the data collection process.
Ethical approval
This study was approved by the Scientific Research and Publication Ethics Committee of Nuh Naci Yazgan University (Date: February 12, 2024, Decision/Protocol No: 2024/002-05). Informed consent was obtained from all participants involved in this study.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors declare that this study received no funding.
Generative AI statement
The authors declare that no generative AI or AI-assisted technologies were used in the writing or preparation of this study.
References
- Singer P, Blaser AR, Berger MM, et al. ESPEN practical and partially revised guideline: clinical nutrition in the intensive care unit. Clin Nutr. 2023;42(9):1671-1689. https://doi.org/10.1016/j.clnu.2023.07.011
- Reber E, Gomes F, Vasiloglou MF, Schuetz P, Stanga Z. Nutritional risk screening and assessment. J Clin Med. 2019;8(7):1065. https://doi.org/10.3390/jcm8071065
- Sáiz-Manzanares MC, Escolar-Llamazares MC, Arnaiz González Á. effectiveness of blended learning in nursing education. Int J Environ Res Public Health. 2020;17(5):1589. https://doi.org/10.3390/ijerph17051589
- Mengi Çelik Ö, Semerci R. Evaluation of nutrition literacy and nutrition knowledge level in nursing students: a study from Turkey. BMC Nurs. 2022;21(1):359. https://doi.org/10.1186/s12912-022-01146-z
- Mancin S, Sguanci M, Cattani D, et al. Nutritional knowledge of nursing students: a systematic literature review. Nurse Educ Today. 2023;126:105826. https://doi.org/10.1016/j.nedt.2023.105826
- Laing BB, Crowley J. Is undergraduate nursing education sufficient for patient’s nutrition care in today’s pandemics? assessing the nutrition knowledge of nursing students: an integrative review. Nurse Educ Pract. 2021;54:103137. https://doi.org/10.1016/j.nepr.2021.103137
- Zubair HM, Yaqoob A, Majeed F, et al. Assessment of nutrition knowledge among university students: a systematic review. Prog Nutr. 2021;23(2):e2021059. https://doi.org/10.23751/pn.v23i2.9374
- Dogan EIK, Borgen I, Ekiz P, Wesseltoft-Rao N. Nutrition education for nursing students: a scoping review. Nurse Educ Today. 2025;144:106460. https://doi.org/10.1016/j.nedt.2024.106460
- Shea A, Brophy L, Nininger J, Abbott M, Wilson L. Nutrition integration across the nursing curriculum: a novel teaching model within a pre-licensure program. J Prof Nurs. 2021;37(6):1162-1166. https://doi.org/10.1016/j.profnurs.2021.10.006
- Benner P. From novice to expert: excellence and power in clinical nursing practice. 1984;84(12):1479. https://doi.org/10.1097/00000446-198412000-00025
- Johnson HL, Owen RP, Romito K, et al. Measuring competency progression across the advanced practice nursing curriculum: a framework for continuous improvement. J Prof Nurs. 2025;61:69-76. https://doi.org/10.1016/j.profnurs.2025.09.011
- Murdoch NL, Epp S, Vinek J. Teaching and learning activities to educate nursing students for interprofessional collaboration: a scoping review. J Interprof Care. 2017;31(6):744-753. https://doi.org/10.1080/13561820.2017.1356807
- Li M, Hong Y, Wu A, et al. The effectiveness of blended learning in nursing and medical education: an umbrella review. Nurse Educ Pract. 2025;86:104421. https://doi.org/10.1016/j.nepr.2025.104421
- Council of Higher Education. Undergraduate nursing curriculum. Ankara: CoHE Publications; 2023.
- American Association of Colleges of Nursing. The essentials: core competencies for professional nursing education. Washington, DC: AACN; 2021.
- Wang A, Wan J, Zhang T, et al. Blended nutrition education with real-life scenarios enhances learning and nutritional counseling capabilities in nursing students. Sci Rep. 2025;15(1):11570. https://doi.org/10.1038/s41598-025-96144-x
- Davis L, Ko A, Turner JA, Gagleard R. Brilliant at the basics part ii: an academic- practice partnership collaboration and its impact on the nursing and health care leadership workforce. J Contin Educ Nurs. 2026;57(1):47-52. https://doi.org/10.3928/00220124-20251009-02
- Bauer S, Eglseer D, Thonhofer N. Assessing malnutrition knowledge in nursing students: a cross-sectional study. Teach Learn Nurs. Published online 2025. doi:10.1016/j.teln.2025.02.026 https://doi.org/10.1016/j.teln.2025.02.026
- Ibrahim RAK, Aldawsari AN. A cross-sectional study of general nutrition knowledge among nursing students in the UAE. J Nutr Metab. 2024;2024:7223610. https://doi.org/10.1155/2024/7223610
- Pleshkan V, Gill M, Gray A, Hall A, Van der Merwe M. An interprofessional health education program developed by nutrition and nursing faculty and students. J Prof Nurs. 2026;63:82-87. https://doi.org/10.1016/j.profnurs.2026.01.002
- Zaghamir DEF, Ibrahim AM. Efficiency of an intervention study on nursing students’ knowledge and practices regarding nutrition and dietary habits. Libyan J Med. 2023;18(1):2281121. https://doi.org/10.1080/19932820.2023.2281121
Copyright and license
Copyright © 2026 The author(s). This is an open-access article under the terms of the Creative Commons Attribution License (CC BY) which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.