
Abstract
Background: The continent of Asia has a vast range of complex nutritional issues ranging from undernutrition and its consequences e.g. anemia, stunting, wasting etc. to overnutrition and its related diseases. Most of the strategies used to combat these health crises are aimed at reducing poverty, increasing food production, and fortifying food. Efforts for identifying sustainable solutions by using existing resources are rare. The reason may be limitations in finding appropriate professional expertise and human resources for these efforts.
Objective: This paper aims to estimate the nutrition profession competence in Asia and to explore its association with food security and the nutrition situation in Asia.
Methods: For comparing State of Nutrition Profession in various countries of Asia four indicators were used: Volume of relevant Research output, Quality of relevant research output, Higher Education opportunities in Nutrition and Country’s Membership international nutrition organizations. Data available at relevant websites was used to collect information about these indicators and a composite index was developed to develop a single variable termed Nutrition Competence Index. Data for Gross Domestic Product (GDP) and Nutritional issues were obtained from the website of the World Bank, and data for food security from Impact Economist. Scale level data was transformed as ranks to represent the relative position of various countries in relation to the study variables. Associations between variables were assessed by studying correlations. Regression analysis was done to estimate the relative role of various indicators in determining the outcome.
Results: The study results indicate that the association between Nutrition research activity score and Food Affordability Score (r=.445, P=.038, n=20) and association between Nutrition Professional Activity Score and Food Availability Score (r=.557, P=.007, n=20) were statistically significant even after controlling for GDP. Similarly, Nutrition research activity scores were found significantly linked with rates of anemia under 5-year-old children (R2 = .52, F(5, 22) = 4.932, p = .004) and rates of stunting under 5-year-old children, (R2 = .58, F(5, 19) = 5.321, p = .003).
Conclusion: It is concluded from this study that Nutrition Competence has the potential to reduce the impact of GDP variations on food security and malnutrition globally, but its strength and utilization vary by continent, particularly in Asia.
Keywords: nutrition competence, GDP, food security, nutrition situation, nutritional issues
Main Points
- Malnutrition remains a public health problem worldwide despite of several nutritional interventional programs.
- Strategies used to reduce the burden of malnutrition usually focusing on alleviating poverty, food fortification, and supplements provision.
- However, despite all these efforts, the area of nutrition education and research is still not in the limelight.
- This research estimated the nutrition profession competence in Asia and also explored its association with food security and the nutrition situation.
- The findings supports that Nutrition Competence has the potential to reduce the impact of GDP variations on food security and malnutrition globally.
Introduction
The realization of the importance of good nutrition as an essential factor for human health as well as sustainable development is increasing.1 The FAO report published in 2019 “Food Security and Nutrition in the World: Safeguarding against Economic Slowdowns and Downturn” clearly demonstrated the association among countries economic status (as assessed by GDP per capita), food security and nutritional status of their populations.2 It is obvious that the level of GDP translates into the personal income of the population, which is the main determinant of the degree to which the population’s needs are satisfied and countries experiencing rapid GDP per capita growth have seen the greatest improvements in food security.3 Unfortunately, the majority of people with food insecurity lives in the Asian regions.4 A sharp increment in food security is observed in developing countries during the last 3 decades and it is alarming that highest number of undernourished people lives in Asia and this continent was a home to 55 percent (402 million) of the people in the world affected by hunger in 2022.5,6 Malnutrition due to limited food availability reflected as stunting and anemia are highly prevalent in Asia.7
It is also noteworthy that in addition to the food access, diet itself is also a contributing factor in the development of many chronic diseases including obesity, cardiovascular disease, hypertension, stroke, type 2 diabetes, metabolic syndrome, some cancers, and perhaps some neurological diseases.8 It is of immense concern that prevalence of these diseases in Asian countries are also escalating that affects the quality of life of people lives in these regions and current studies revealed the metabolic risk factors including obesity, and overweight population mostly with central obesity.9 To overcome these health crises, strategies employed were largely targeted to reduce poverty to make possible the availability of food to the population, to increase food production, and food fortification to optimize food utilization. The current analysis expands on our earlier investigation into the relationship between food security and nutrition competence and the role of GDP in predicting nutritional issues across Asian countries.10
Nutrition professionals play a pivotal role not only in addressing the epidemiological aspects of nutrition-related diseases but also in enhancing access to social, health, and basic services. Consequently, the presence of professionals with an academic background in nutrition within the public health field offers a promising resource for the formulation of action plans aimed at eradicating these nutritional concerns. Furthermore, their involvement in emergency preparedness and response efforts, capacity building, and training initiatives underscores the breadth of their impact. In times of crisis, nutrition professionals can ensure access to nutritious food and essential services, mitigating the effects on nutrition-related health outcomes. Overall, their expertise and engagement are essential for developing targeted and effective action plans that encompass a wide range of social, health, and basic service considerations, ultimately working towards the eradication of nutritional concerns. Certainly, the inclusion of nutritionists in multidisciplinary teams is imperative, given their academic expertise and understanding of diseases linked to diet. Their ability to suggest preventive measures and treatment options adds significant value to such teams.11
This study aimed (i) to estimate the nutrition profession competence in Asia, (ii) to explore the association of nutrition competence with food security and nutrition situation in Asia and (iii) to elucidate the potential of nutrition competence in determining the benefit from higher income of countries.
Methodology
Study Variables and Data Resources: This research is based on the use of secondary data in which information about the countries was retrieved from documents and statistics publicly available on the websites of international organizations. In this study, groups of variables related to GDP and food insecurity as a predictor of nutritional issues in Asian countries as well as to develop nutritional competence were carefully selected. The prime source of data for information about GDP and Nutritional issues (including Anemia in under 5-year child, Hypertension, overweight in Adults and children, severe Wasting Under 5, Stunting Under-5, Undernourished Population and wasting Under-5) in Asian countries is taken from the website of “The World Bank” and information about the indicators to assess the status of food insecurity in these countries was extracted from the website of “Economist Impact”.12,13
Measurement of Nutrition Profession Index: The estimation of Countries’ Nutrition Profession status was done by assessing commitment to and competence in the field of nutrition. “Participation in nutrition activity” and “availability of higher education opportunities in nutrition” indicated commitment while research output and quality of research output indicated competence. Counties were ranked on these parameters in tertiles and sum of scores on these variables was used as Nutrition Profession Index. Higher scores were expected to indicate higher action potential. Validity of the index was judged by using the publication of national food based dietary guidelines as an outcome variable. NPI of countries that have published or not published NFBDG was compared and was found to be significantly higher P=0.029 for countries that have published NFBDG (8.2) as compared to those that have not published NFBDG (6.8).
(i) Nutrition Higher Education Score in which proportion of Higher Education Institutes in a country that are offering nutrition degree programs (Number of institutions offering nutrition/total number of HEIs listed in World higher Education Database) https://www.whed.net/home.php. (ii) Nutrition research Excellence Score: H-Index of all the Scholars from any country that are listed in AD scientific Index as Scientists in the field of Nutrition and Dietetics https://www.adscientificindex.com. (iii) Nutrition research Activity Score: Research output was estimated by comparing the number of scientific publications in the past 5 years in the area of human Nutrition in Google Scholar. The ratio of population to number of publications and Nutrition Research Activity Score (NRAS) was generated by converting this information to normal scores. (iv) Nutrition Professional Activity Score: Information about membership of country’s nutrition organizations in international bodies i.e. the International Union of Nutritional Sciences (IUNS), the International Confederation of Dietetic Associations (ICDA) and International Affiliate of the Academy of Nutrition and Dietetics (IAAND) was retrieved from relevant websites and scores were assigned according the number of bodies in which country’s nutrition bodies participated.14,15,16
Data Analysis: Data was analyzed using SPSS version 20. Scale level data was transformed as ranks to represent the relative position of various countries in relation to the study variables. Countries were categories in groups to study associations with indictors having data as categories. Associations between variables was assessed via Pearson correlation. Multiple Linear Regression analysis was done to estimate the relative role of various indicators in determining the outcome.
Results
1. Nutrition competence in Asia
Status of the Nutrition competence is Asia among six continents were presented as:
(i) State of Nutrition Focus in HEIs in Asia
Table 1 and Table 2 provides basic descriptive statistics of the proportion of HEIs with Nutrition programs in various continents. Results shows that Asia ranked 5th among 6 continents (Table 1) with HEIs with Nutrition programs and among 42 countries in Asia 12 countries are those which does not has the Nutrition programs in their universities (Table 2).
| Table 1. Mean proportion of HEIs with nutrition programs in various continents | ||||||
| Continent Name |
|
|
|
|
|
|
| Mean |
|
|
|
|
|
|
| SD |
|
|
|
|
|
|
| Table 2. Proportion of countries having various percentage of HEI with nutrition programs | ||||||||
| Continent name |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
| Africa |
|
|
|
|
|
|
|
|
| Asia |
|
|
|
|
|
|
|
|
| Europe |
|
|
|
|
|
|
|
|
| North America |
|
|
|
|
|
|
|
|
| Oceania |
|
|
|
|
|
|
|
|
| South America |
|
|
|
|
|
|
|
|
(ii) Nutrition research output and Excellence in Asia
Dietetic research output
Table 3 represents the distribution of dietetics research output (score based on the ratio of continent’s population to number of publications in Nutrition in the past 5 years) across different continents. The table shows the number of dietetic research outputs at three different levels: low, medium, and high. According to the results Africa has highest research output (54) among other continents. Asia has second highest rate of dietetic research output (51) among others in which 17 were at the low level (33.3% of the total), 16 were at the medium level (31.4% of the total), and 18 were at the high level (35.3% of the total). Whereas, least was observed in South America.
| Table 3. Dietetic research output | ||||||
| Continent name |
|
|||||
|
|
|
|
||||
|
|
|
|
|
|
|
|
| Africa |
|
|
|
|
|
|
| Asia |
|
|
|
|
|
|
| Europe |
|
|
|
|
|
|
| North America |
|
|
|
|
|
|
| Oceania |
|
|
|
|
|
|
| South America |
|
|
|
|
|
|
Nutrition research excellence
Table 4 shows that countries in continent Oceania actively contribute to promoting Nutrition research than others. Asia ranked 3rd in Nutrition Research excellence with moderate number of researchers in this field (13.44), number of research institute (15.55) and mean H-index of researchers (21.53).
| Table 4. Nutrition research excellence | ||||||
| Reserch parameters |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Number of Researchers |
|
|
|
|
|
|
| Number of Institutions |
|
|
|
|
|
|
| Mean H INDEX of Researchers* |
|
|
|
|
|
|
(iii) Nutrition Professional Activity in Asia:
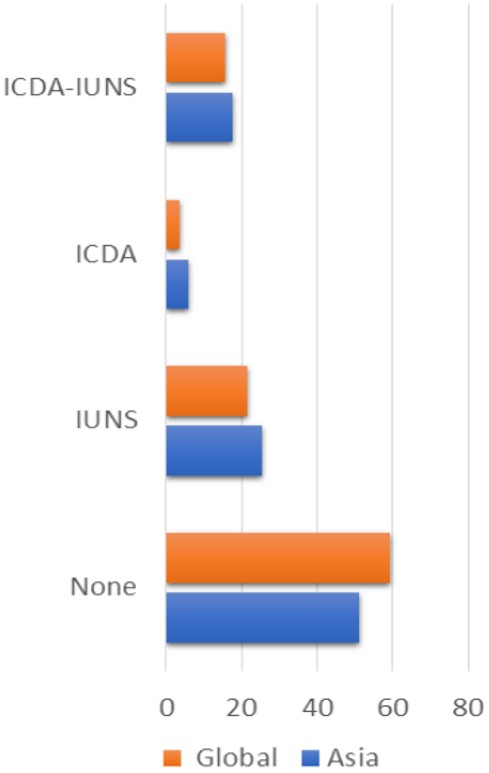
Nutrition profession activity score was measured from number of memberships of country’s nutrition organizations in international bodies (IUNS, ICDA and IAAND) (Figure 1) and results revealed that among 51 countries in Asia 25 countries has memberships with Nutrition related international organizations (Table 5).
| Table 5. Membership of countries from Asia in international organizations | ||||||||
|
|
|
|||||||
|
|
|
|
|
|
|
|||
| None | Count |
|
|
|
|
|
|
|
| % |
|
|
|
|
|
|
|
|
| IUNS | Count |
|
|
|
|
|
|
|
| % |
|
|
|
|
|
|
|
|
| ICDA | Count |
|
|
|
|
|
|
|
| % |
|
|
|
|
|
|
|
|
| ICDA-IUNS | Count |
|
|
|
|
|
|
|
| % |
|
|
|
|
|
|
|
|
| Total | Count |
|
|
|
|
|
|
|
| % |
|
|
|
|
|
|
|
|
2. Nutrition competence index:
Overall, all four indicators to assess Nutrition competence in Asia shows a positive correlation (Table 6).
| Table 6. Association between nutrition competence indicators | |||||
|
|
|
|
|
||
| Nutrition professional activity score | Pearson Corr. |
|
|||
| Sig. (2-tailed) |
|
|
|||
| N |
|
|
|||
|
Nutrition higher education score
|
Pearson Corr. |
|
|
||
| Sig. (2-tailed) |
|
|
|
||
| N |
|
|
|
||
|
Nutrition research excellence score
|
Pearson Corr. |
|
|
|
|
| Sig. (2-tailed) |
|
|
|
|
|
| N |
|
|
|
|
|
| Nutrition research activity score | Pearson Corr. |
|
|
|
|
| Sig. (2-tailed) |
|
|
|
|
|
| N |
|
|
|
|
|
3. Association of nutrition competence with food security and nutrition situation in Asia
Table 7 shows a positive, statistically significant correlations (p<0.01and p<0.05) were observed between the Nutrition Competence Index and food security score (r=0.568), Food Affordability Score (r =0.505), Food Availability Score (r = 0.543) and Food Quality Score (r=0.411). Table 7 also indicted the significant positive association (p<0.01) between Nutrition research Excellence Score with Food Security Score (r=0.591), Food Affordability Score (r=0.565) and Food Quality Score (r=0.564) even after controlling for GDP.
|
**. Correlation is significant at the 0.01 level (2-tailed). *. Correlation is significant at the 0.05 level (2-tailed). |
||||||
| Table 7. Association between countries’ nutrition competence and food security indicators in Asia | ||||||
|
|
|
|
|
|
||
| Food security score | Pearson Cor. |
|
|
|
|
|
| N |
|
|
|
|
|
|
| Food affordability score | Pearson Cor. |
|
|
|
|
|
| N |
|
|
|
|
|
|
| Food availability score | Pearson Cor. |
|
|
|
|
|
| N |
|
|
|
|
|
|
| Food quality score | Pearson Cor. |
|
|
|
|
|
| N |
|
|
|
|
|
|
| Food resilience score | Pearson Cor. |
|
|
|
|
|
| N |
|
|
|
|
|
|
Association between Countries’ Nutrition Competence & Nutrition Relevant Indicators in Asia are presented in Table 8. After controlling for GDP, It is clear that, hypertension had significant negative correlation with Nutrition Higher Education Score (r=-0.410, P=0.0129) and marginally significant correlation with Nutrition Professional Activity Score (r=-0.321, P=0.055). Undernourishment had significant positive correlation with Nutrition research activity (r=0.371, P=0.026). Wasting Under-5 had significant positive correlation with Nutrition Professional Activity Score (r=0.333, P=0.046).
|
**. Correlation is significant at the 0.01 level (2-tailed). *. Correlation is significant at the 0.05 level (2-tailed). |
|||||
| Table 8. Association between countries’ nutrition competence & nutrition relevant indicators in Asia | |||||
|
|
|
|
|
|
|
|
|
|||||
| Anemia Under 5 Child |
|
|
|
|
|
| Hypertension |
|
|
|
|
|
| Overweight Adults |
|
|
|
|
|
| Overweight Child |
|
|
|
|
|
| Severe Wasting Under 5 |
|
|
|
|
|
| Stunting Under-5 |
|
|
|
|
|
| Undernourished Population |
|
|
|
|
|
| Wasting Under-5 |
|
|
|
|
|
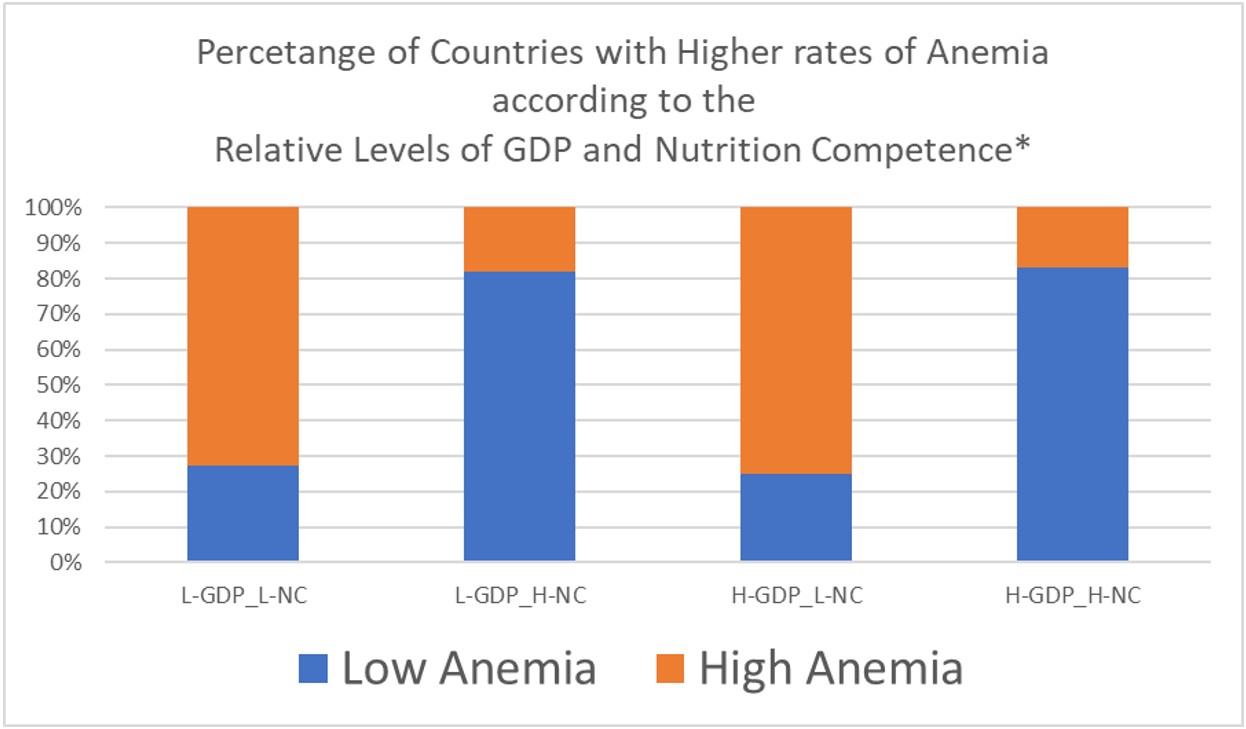
The relationship between GDP, Nutrition Competence, and the prevalence of anemia among children under the age of 5 is shown in Figure 2. The data suggests that higher GDP is associated with lower prevalence of anemia, while higher nutrition competence is also associated with lower prevalence of anemia. Additionally, the data shows that there are significant differences in the prevalence of anemia between different GDP and nutrition competence groups. Table 9 (a) and Table 9 (b) shows the Nutrition Competence Variables as predictor of anemia and stunting under five years of age. Nutrition research activity scores predicted Rates of Anemia under 5-year-old children, R2 = .52, F(5, 22) = 4.932, p = .004 (Table 9 a). Nutrition research activity scores predicted Rates of STUNTING under 5-year-old children, R2 = .58, F(5, 19) = 5.321, p = .003 (Table 9 b).
| Table 9. (a). Nutrition competence variables as predictor of nutritional issues (Anemia) | ||||||
| Coefficients | ||||||
| Model |
|
|
|
|
||
|
|
|
|
||||
| 1 | (Constant) |
|
|
|
|
|
| GDP.PC |
|
|
|
|
|
|
| Nutrition Higher Education Score |
|
|
|
|
|
|
| Nutrition research Excellence Score |
|
|
|
|
|
|
| Nutrition research activity score |
|
|
|
|
|
|
| Nutrition Professional Activity Score |
|
|
|
|
|
|
| (b). Nutrition competence variables as predictor of nutritional issues (Stunting) | ||||||
| 1 | (Constant) |
|
|
|
|
|
| GDP.PC |
|
|
|
|
|
|
| Nutrition Higher Education Score |
|
|
|
|
|
|
| Nutrition research Excellence Score |
|
|
|
|
|
|
| Nutrition research activity score |
|
|
|
|
|
|
| Nutrition Professional Activity Score |
|
|
|
|
|
|
Discussion
Many factors influences the health status of individuals in a population. These factors ranges from country level aspects e.g. GDP.PC, food security conditions, investment in the health care system to household level e.g. dietary practices, hygienic conditions etc. The effect of these elements on health issues has already been extensively studied. The positive impact of economic growth on increased life expectancy and lower infant mortality has already been established.17
But besides these, there is also an important element that is still neglected i.e. Nutrition competency. The most common nutrition competencies includes skills in nutrition assessment, the ability to prescribe dietary interventions in the prevention and treatment of disease, knowledge of the role of nutrition in health promotion and disease prevention and knowledge of the social and cultural importance of food, including food consumption trends and current nutrition recommendations.18 In this study nutrition competencies among various continents were measured on the basis of number of HEI with Nutrition programs, Nutrition research excellence and Nutrition Professional Activity. Our results showed that South America has highest number of HEI among other continents. This continent ranked 4th in the list of by GDP per capita (PPP) provided by International Monetary Fund in 2023. The continent Oceania (ranked 2nd in 2023 list of GDP.PC provided by IMF) has highest score in Nutrition Research Excellence with highest number of researchers, Institutions and mean H INDEX of researchers. As far as continent Asia is concerned, it ranked 5th in having Higher Education Institutes with Nutrition programs among other continents and has second highest rate of dietetic research output with a significant level of memberships in Nutrition related International organizations.
It is obvious from the current study that even countries with low GDP and high Nutrition competence has low rate of anemia in under 5 years old children (Figure 2) as compared to the countries with high GDP but with low nutrition competence. Similarly, our results also suggested that countries with high GDP but low nutrition competence has high ratio of stunting among children under 5 years of age (26.26) as compared to those countries with high GDP but low nutrition competence (10.32). Previous studies clearly demonstrated the effect of nutrition knowledge on prevalence of anemia in pre-school children and stunting in the same age group.19,20 Our finding indicates that GDP per capita (GDP.PC) has a negative standardized coefficient of -.405, indicating that as GDP per capita increases, the rates of anemia in children decrease. Moreover, the nutrition research activity score has a negative standardized coefficient of -.449, indicating that as the nutrition research activity score increases, the rates of stunting in children decrease. Overall, the results suggest that the nutrition research activity score is a significant predictor for both anemia and stunting rates in under 5-year-old children, while the other variables do not show significant relationships. Our findings provide strong evidence of the positive impact of nutrition research activity on nutritional issues.
Conclusion
Globally and more so in Asia, the Nutrition Competence has potential to decrease the impact of variations in GDP on food security and Malnutrition however there are continent wise variations in strength and utilization of this potential. But presence of NC alone may not give the optimum benefits if there is no assurance of utilization of competence. Challenges in estimation of nutrition competence and flexibilities in human resource management are probably the biggest hindrance in capacity building and capacity utilization.
Strength and Weaknesses
The comprehensive data sources and a multidimensional approach to measuring nutrition competence provide strength in data collection. The use of standardized coefficients and numerical values, such as the negative coefficients for GDP per capita and nutrition research activity score, adds precision to the findings. This quantitative approach enhances the objectivity and reliability of the study. However, limitations can be in the potential data limitations only secondary sources are used, considering the exclusivity of data sources, “The World Bank” and “Economist Impact” might introduce a bias, minimizing subjectivity in scoring, as scoring criteria is missing, which can create the bias, study period is only five years, which can be considered as a limitation.
Ethical approval
The study did not require ethical approval as it was based on secondary data analysis.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Thow AM, Farrell P, Helble M, Rachmi CN. Eating in developing Asia: trends, consequences, and policies. Wellness for a Healthy Asia. 2021;19,107.
- FAO, IFAD, UNICEF, WFP, WHO. The state of food security and nutrition in the world 2019: safeguarding against economic slowdowns and downturns. Rome: FAO; 2019:1-219 Available at: https://openknowledge.fao.org/items/f73edb75-4017-497b-8ca3-e66ea2109560
- Świetlik K. Economic growth versus the issue of food security in selected regions and countries worldwide. Problems of Agricultural Economics. 2018;3:127-148. https://doi.org/10.30858/zer/94481
- Abdullah, Qingshi W, Akbar M. A spatial panel analysis of food security and political risk in Asian countries. Social Indicators Research. 2022;161:345-378. https://doi.org/10.1007/s11205-021-02821-5
- Mahmood T, Kumar R, Ali TM, Naeem N, Pongpanich S. Determinants of the food insecurity at household level in Pakistan: a multilevel model approach. PLoS One. 2023;18:e0291343. https://doi.org/10.1371/journal.pone.0291343
- FAOSTAT F. Suite of food security indicators. Rome, Italy: Food and Agriculture Organization (FAO). 2023; Available at: http://www.fao.org/faostat/en/#data/FS (Accessed on Jul 12, 2023).
- Khan Z, Ali A. Global food insecurity and its association with malnutrition. Emerging Challenges in Agriculture and Food Science. 2023;8:2-19. https://doi.org/10.9734/bpi/mono/978-81-19217-36-6/CH1
- Gropper SS. The role of nutrition in chronic disease. Nutrients. 2023;15:664. https://doi.org/10.3390/nu15030664
- Biswas T, Townsend N, Gupta RD, et al. Clustering of metabolic and behavioural risk factors for cardiovascular diseases among the adult population in South and Southeast Asia: findings from WHO STEPS data. Lancet Reg Health Southeast Asia. 2023;12:100164. https://doi.org/10.1016/j.lansea.2023.100164
- Hakeem R, Herrera M, Jahan M. Food security and nutrition competencies diminish the role of GDP in predicting stunting variations among countries. Nurture. 2023; 17,427-438. https://doi.org/10.55951/nurture.v17i3.362
- Román AC, Villar MA, Belmont-Guerron P, Ocampo MB. Undervalued professionals: placement of nutritionist in the Ecuadorian health system. BMC Health Serv Res. 2023;23:407. https://doi.org/10.1186/s12913-023-09340-8
- The World Bank. Available at: https://www.worldbank.org
- Economist Impact. Available at: https://impact.economist.com.
- IUNS: The International Union of Nutritional Sciences, Available at: https://iuns.org/
- ICDA: The International Confederation of Dietetic Associations. https://internationaldietetics.org/
- IAAND: International Affiliate of the Academy of Nutrition and Dietetics. Available at: https://eatrightinternational.org/
- Majeed MT, Gillani S. State capacity and health outcomes: an empirical analysis. Pak J Commer Soc Sci PJCSS. 2017; 11:671-697
- Lepre B, Mansfield KJ, Ray S, Beck EJ. Nutrition competencies for medicine: an integrative review and critical synthesis. BMJ Open. 2021;11:e043066. https://doi.org/10.1136/bmjopen-2020-043066
- Alamneh TS, Melesse AW, Gelaye KA. Determinants of anemia severity levels among children aged 6-59 months in Ethiopia: multilevel bayesian statistical approach. Sci Rep. 2023;13:4147. https://doi.org/10.1038/s41598-022-20381-7
- Marume A, Archary M, Mahomed S. Predictors of stunting among children aged 6-59 months, Zimbabwe. Public Health Nutr. 2023;26:820-833. https://doi.org/10.1017/S1368980023000046
Copyright and license
Copyright © 2025 The author(s). This is an open-access article under the terms of the Creative Commons Attribution License (CC BY) which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.
